

EXECUTIVE SUMMARY
In furtherance of our mission, we offer the following recommendations that we hope will serve as a blueprint for action for policymakers on both the federal and state levels in 2021 and beyond.
This document is divided into three sections, each of which speak to the underlying goals of increasing access to reproductive medicine, particularly treatment and care related to a diagnosis of Infertility; ensuring that all Americans - regardless of demographics - have access to medical care that supports family building; and committing to an increased investment in a robust national research agenda that prioritizes reproductive medicine.
Our specific recommendations, as discussed in detail in the pages that follow, are:
Goal I: Expanding Access to Reproductive Medicine, Particularly Infertility Care
- Pass a National infertility coverage insurance mandate. Specifically, require all health plans offered in group and individual markets (including Medicaid, EHBP, TRICARE, VA) to cover infertility treatment.
- Expand research on reproductive-related conditions and diseases (infertility, maternal and gynecological health, etc.) across federal agencies, including the NIH’s Office for Women’s Health Research and work within these agencies to establish innovative programs to expand access to care and services (e.g., a Federal Access to Contraception Program to address gaps in access for those whose employers may not offer contraceptive coverage).
- Establish permanent Infertility Benefits for Active-Duty Members of the U.S. Military, Veterans, and Employees of the Veteran’s Administration.
Goal II: Addressing Unique Barriers to Reproductive Medicine for Specific Populations
- Pass a National mandate to enforce insurance coverage for fertility preservation for those at-risk of iatrogenic infertility
- Develop and implement HHS/DOJ/EEOC rule to protect sub-populations from discrimination in infertility coverage
- Increase funding for increased reproductive health education for students in middle and high schools, colleges and universities, medical schools and postgraduate medical training
- Fund and require cultural bias and sensitivity training for all medical providers
Goal III: Increasing the National Investment in Reproductive Medicine-Related Research
- Increase funding for research in human reproductive disorders. Specifically, increase funding for the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD)
- Lift the prohibition on human embryo research and allow the National Institutes of Health (NIH) to develop oversight of the ethics of research proposals
- Protect, through Congressional codification, access to embryonic stem cell lines
- Protect, through Congressional codification, access to fetal cell lines
- Authorize the FDA to examine the data of any proposed germ line gene editing techniques
INTRODUCTION
REPRODUCTIVE HEALTH CARE: A NATIONAL PRIORITY THAT CANNOT WAIT
Infertility, recognized by the American Medical Association and the World Health Organization as a disease that impacts as many as 7.3 million couples in the United States, can, untreated, upend the dream of building a family. For many, the ability to become a parent hinges on affordable access to in vitro fertilization (IVF), a treatment that has been safely practiced in America for nearly five decades. The disease of infertility does not discriminate, impacting Americans regardless of race, age, ethnicity, sexual orientation or economic status.In IVF, eggs are fertilized in a lab to increase the likelihood of pregnancy. Microscopic, fertilized eggs are then transferred to a woman’s uterus in hope that they will lead to a successful pregnancy. Myriad medical procedures and advancements exist to address individual challenges to pregnancy, as well as comorbidities.
To be clear: Reproductive medicine encompasses much more than Infertility. In fact, reproductive medicine is a branch of medicine that also addresses issues related to puberty, menopause, contraception, and related medical conditions. As the boundaries of fertility research have expanded, so, too, has ASRM’s focus. This is reflected both in ASRM’s growing and diverse membership, as well as our structure. For example, in 2018, the ASRM Research Institute was founded. Funding from the Institute enables researchers to explore relevant topics, such as basic human gametes and endocrinology. While this document and our recommendations center largely on the needs of individuals diagnosed with Infertility and the medical professionals who work to support and treat them, ASRM’s focus remains a broad one.
In this document, we provide background and recommendations for federal policy reforms to advance the following three overarching goals:
Goal I: Expanding Access to Reproductive Medicine, Specifically Infertility Services
Goal II: Addressing Unique Barriers to Access and Care for Specific Populations
Goal III: Increasing the National Investment in Research into Reproductive Medicine
DISCUSSION
GOAL I: PROTECT AND EXPAND ACCESS TO REPRODUCTIVE MEDICINE
For one in eight couples in America, the diagnosis of Infertility can kill the dream of becoming parents. When we speak of a desire to expand access to reproductive medicine, we’re really talking about a desire to ensure that all Americans, regardless of their zip code, race, socioeconomic background, sexual preference, or the like can take advantage of the incredible scientific advances our members use every day to support family building. Below, we discuss some of the common challenges Americans diagnosed with Infertility experience and offer policymakers concrete suggestions for cost-effective, common-sense policy reforms that could prove to be all the difference for some families.Passing a federal infertility insurance mandate is key to ensuring equitable access to affordable fertility care.
Barriers to Care and Coverage
Despite gradual strides at both the state and national levels in the last decade, cost and access remain significant barriers to many couples’ ability to use reproductive medicine to build their families. Fertility treatments are expensive and whether or not they will be covered by insurance can be dependent upon one’s economic status, zip code or employer. For example, while private insurance carriers have, in many instances, stood up to cover diagnostic services, fewer cover the more expensive aspects of infertility care, including procedures such as IVF and Intrauterine Insemination (a fertility treatment involving the placement of sperm inside a woman’s uterus close to the Fallopian tubesin order to increase chances of conceiving). Sixty-seven percent of patients report spending $10,000 or more to build their families.
State Laws and Policies on Infertility
In recent years, with increased awareness of, and demand for, infertility care, states have taken decisive action to expand access to care. This reflects an understanding that increasing individuals’ ability to start a family is sound policy: People who need IVF and have employer-provided infertility health insurance protections express a higher rate of overall satisfaction with their employer.1While this is all promising, our work is far from over. Currently, only 17 of 50 U.S. states have infertility care insurance mandates, which are assumed to increase accessibility of those services, but recent research finds employers determine the applicability of state mandates.
Recently, researchers from the University of South Florida in Tampa performed 66 interviews with women and men ages 18-45. The selection of interview questions reflects the hypothesis that residence, employer, and presence and type of health insurance affect the decisions people make regarding when, how, and to what extent they access infertility services.2
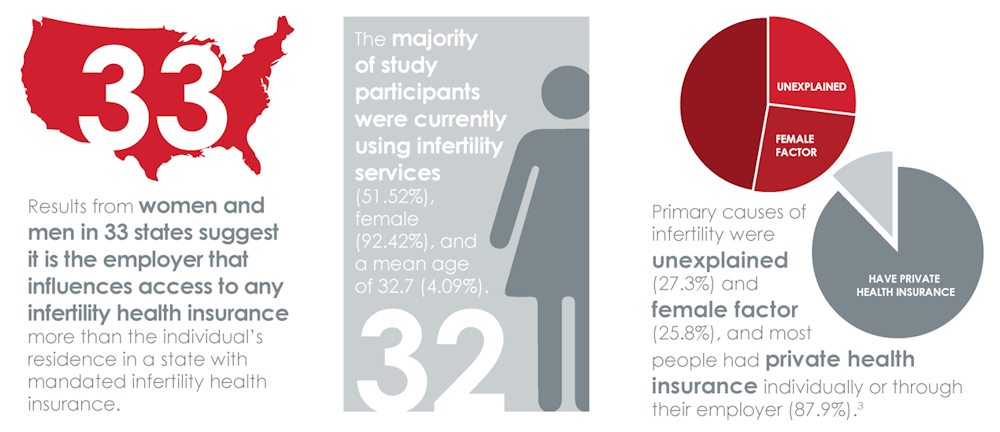
The majority of study participants were currently using infertility services (51.52%), female (92.42%), and a mean age of 32.7 (4.09%). Primary causes of infertility were unexplained (27.3%) and female factor (25.8%), and most people had private health insurance individually or through their employer (87.9%).3
Although state insurance mandates exist to support coverage of fertility care, the unfortunate reality is that your employer, not your state, may determine your access to affordable fertility care. While some employers embrace the opportunity to support their employees’ family building dreams, others take advantage of Federal loopholes and create hurdles instead of bridges to care. In fact, most IVF patients pay out of pocket for care, which can cost thousands of dollars per cycle. And while some states have, in recent years, taken laudable steps to increase access to infertility care, only a fraction of states require private insurance plans to cover infertility services. Moreover, with only one state currently mandating coverage under Medicaid, the financial barriers to infertility care for low-income citizens can be all but impossible to overcome. We are failing Americans if the opportunity to build a family is more likely to be determined by one’s bank account balance than legitimate medical concerns.
According to the ASRM Ethics committee, economic barriers are not the only impediments to accessing infertility care.4 Chief among non-economic barriers are cultural and societal factors. Researchers who have studied African American, Hispanic, Muslim, and Asian populations in the United States have noted that communication differences, cultural stigmas (including male and female aversion to being labeled infertile), cultural emphasis on privacy, and unfamiliarity or prior bad experiences with the U.S. medical system can dissuade members of certain racial, ethnic, or religious groups from seeking care for infertility.5 Language differences also may discourage non–English-speaking patients from seeking care.
Another obstacle is the burden of pursuing infertility treatment, particularly cycle-based therapies like in- vitro fertilization (IVF). In addition to cost barriers, infertility patients often must take substantial time away from work for repeated office visits and associated procedures, and must be able to travel to medical facilities, which are often geographically distant.6 Additionally, many treatments require repeated cycles and the ability to follow complex medical instructions.7
Another obstacle is the burden of pursuing infertility treatment, particularly cycle-based therapies like in- vitro fertilization (IVF). In addition to cost barriers, infertility patients often must take substantial time away from work for repeated office visits and associated procedures, and must be able to travel to medical facilities, which are often geographically distant.6 Additionally, many treatments require repeated cycles and the ability to follow complex medical instructions.7
Other patients may be denied access to effective care if the institution at which they seek treatment does not inform them of the availability of certain treatment options, such as IVF, because they conflict with the religious affiliation of the facility. Fair access also is impaired by providers who refuse to treat unpartnered individuals and same-sex couples, a practice that ASRM rejects.8
Americans’ demand for access to reproductive medicine and related care continues to grow. According to a 2020 analysis from the Kaiser Family Foundation (which reviewed the 2015-2017 National Survey of Family Growth (NSFG)), 10% of women ages 18-49 say they or their partner have spoken with a physician about ways to help them become pregnant. Moreover, the CDC has noted a steady increase in the use of IVF since its first successful birth in 1981. As also reported by the Kaiser Family Foundation, an estimated 1.8% of U.S. infants are conceived annually using assisted reproductive technology (ART, which includes IVF).9
An Opportunity for America to Lead on Access to Reproductive Medicine
ASRM is committed, in partnership with other state and local stakeholders, to continued advocacy for state laws to increase access to reproductive care. That said, it is clear that these measures alone are not enough. Passing a federal infertility insurance mandate is key to ensuring equitable access to affordable fertility care.In recent years, several measures have been introduced, with bipartisan support, to ensure that members of our Federal workforce have access to comprehensive, affordable infertility treatment and care. For example, the Infertility Treatment and Care Act (S. 1641/H.R. 2803) would provide those who receive their health care through government-sponsored health plans, including TRICARE, the VA, the Federal Employee Health Benefits Program, and others would have coverage for infertility services. Importantly, as has been an increasing trend at the state level and one we wholeheartedly support, this legislation will provide access to vital fertility preservation services for those, like cancer patients and wounded warriors (as discussed in more detail elsewhere in this document), who are at risk of infertility due to medical treatments such as chemotherapy and surgery.
Initiatives like this present an opportunity for the United States to assert itself as an international leader in the provision of infertility coverage to countless civil servants whose dream of family building may be stalled with these bills in Congress. We welcome the opportunity to work with the Biden Administration to achieve this and related goals.
Access to Contraception
In keeping with our belief that women have the right to make informed and autonomous healthcare decisions, ASRM is closely monitoring litigation surrounding the Affordable Care Act’s (ACA) contraception mandate.In July 2020, the United States Supreme Court held that employers with a religious or moral objection to providing contraception coverage to their employees may opt out of the requirement with impunity. As Justice Ginsburg pointed out in her dissent to the 7-2 majority opinion (Little Sisters of the Poor Saints Peter and Paul Home v. Pennsylvania, No. 19-431 (U.S. Jul. 8, 2020), the government has estimated between 70,500 and 126,400 women would lose access to no-cost contraception under the broadening of this exemption. Notably, she said in her dissenting opinion:
This Court leaves women workers to fend for themselves, to seek contraceptive coverage from sources other than their employer’s insurer, and, absent another available source of funding, to pay for contraceptive services out of their own pockets.
Particularly in the midst of a global pandemic, it is alarming to contemplate the potential impact of the Supreme Court’s decision and the rules and policies put forth by its proponents: the loss of no-cost birth control for up to hundreds of thousands of women would be devastating. These points are particularly salient with women of color and who are low-income, poised to be among the hardest hit. As Justice Ginsburg further noted:
More than 2.9 million Americans—including approximately 580,000 women of childbearing age—receive insurance through organizations newly eligible for this blanket exemption. Of cardinal significance, the exemption contains no alternative mechanism to ensure affected women’s continued access to contraceptive coverage.
As we await a final decision from the highest Court as to the ACA’s overall Constitutionality (arguments are taking place at the time of publication), we urge the Biden Administration to take meaningful steps to ensure that, to the greatest degree possible, access to low or no-cost contraception remains a priority.Complicating matters even further in terms of efforts to ensure access to contraceptive care have been archaic procedural requirements that limit access to contraception as an over-the-counter medication. As recently discussed at length in a piece published in the Journal of the American Medical Association (JAMA), efforts have long been underway (and stymied) on both the state and federal levels to eliminate requirements for in-person medical appointments for purposes of obtaining contraception. While, historically, such requirements may have made sense, decades of research and experience have informed the drive to expand access through a transition from prescription-only to over-the-counter access to contraceptives.
Legislation on the federal level designed to expand patient access to contraception has routinely stalled, with states and non-profit organizations, such as Planned Parenthood, stepping in to, for example, allow patients to obtain contraceptives via online services subject to review by a licensed medical professional.
Particularly in the time of COVID-19, when so many are reliant on telemedicine and unable or unwilling to travel to in-person appointments, these efforts have proven valuable. Unfortunately, the sustainability of such programs is questionable. As reported in JAMA, at least 18 states have banned the use of telemedicine for the provision of drugs to effectuate medical abortions. We join our colleagues at fellow national medical organizations in urging policymakers to identify and prioritize safe, common-sense measures to ensure unhindered over-the-counter access to contraception.
Access to Abortion
ASRM has joined with colleagues from other leading medical organizations and societies, including the American Medical Association and the American College of Obstetricians and Gynecologists, in challenging any efforts to restrict access to abortion, a safe, proven medical procedure. This is in keeping with ASRM’s legacy of working to ensure that women face fewer barriers to receiving legal health care, and to advance and support policies that guarantee women’s rights to control their reproductive health choices.Most recently, ASRM raised questions, in the course of Justice Amy Coney Barrett’s nomination to the Supreme Court, regarding the potential impact of her (as yet unclear) views on IVF to patients and providers alike. As our President, Hugh Taylor, M.D., explained in a letter to U.S. House leaders:
Judge Coney Barrett has not offered clarity on her views [of IVF, cryopreservation of eggs] and related family building procedures… We do not, yet, know if she is opposed to the resulting embryos from an IVF procedure being either frozen for future use or discarded, based on the family plan created by the intended parents and their physician. We do not know if she endorses the concept that any process which results in an embryo created outside of a uterus has the same inalienable rights as you and I, and, therefore, whether she would oppose the ability of an individual or couple to choose if and when to implant said embryo.
While the nuances of each case vary, we have joined fellow experts (through Amicus briefs, public statements, and the like) with a vested interest in our patients’ well-being and fulfillment of our professional duty, in challenging assertions that there is a specific medical need to limit access to abortion generally and, specifically, during the time of COVID-19.
On the point of the pandemic, it is our belief, as medical experts, that the pandemic does not justify restricting or prohibiting abortion care. In fact, we have joined fellow national experts in asserting that such orders to restrict abortion care will increase, rather than decrease, use of already strained hospital resources and precious personal protective equipment.
Seamless and Equitable Access to Third-Party Pregnancy Options
Earlier this year, ASRM sent a letter to Secretary of State Mike Pompeo requesting limited but critical exceptions to sweeping travel restrictions that have directly impacted families whose dreams of parenthood hinge on the ability to travel and connect with their surrogates. Currently, nine out of 10 people are living in countries that have closed their borders due to COVID-19.ASRM recognizes that these are, in many ways, unprecedented times and call for serious measures to protect individuals’ health and safety. That said, we are urging the State Department to carve out a narrowly tailored surrogacy exception to allow children who are born in the U.S. to return home with their parents. The unintended consequences of travel bans on family building are being globally felt. In May 2020, it was reported that at least 100 infants born through surrogacy, some to intended parents from the United States, are in limbo, waiting in hospitals for parents desperate to travel to and care for them. In the Ukraine alone, officials estimate as many as 1,000 expectant surrogate mothers may give birth before restrictions are lifted, making action to allow for parents to travel from the United States to their infants all that more necessary and time sensitive.
Under current law, even babies born to gestational surrogates on U.S. soil are required to attain a U.S. passport to exit the country. Allowing for intended parents to enter the United States with all due health precautions and creating an exception for newborns born through surrogacy during the COVID-19 pandemic to obtain passports are reasonable and sound steps. These steps will ensure that parents can be present for a child’s birth to take physical and legal responsibility for their children and, as applicable and only when deemed safe, return home to an International location as a family. Without exception, these children are at risk of being trapped in the U.S., potentially without a legal guardian or health insurance. In fact, we would encourage lawmakers to consider extending such measures to non-COVID times as appropriate.
Recommendations to Expand Access to Infertility Services/Reproductive Medicine
- Pass a National infertility coverage insurance mandate. Specifically, require all health plans offered on group and individual markets (including Medicaid, EHBP, TRICARE, VA) to cover infertility treatment.
- Expand research on reproductive-related conditions and diseases (infertility, maternal and gynecological health, etc.) across federal agencies, including the NIH’s Office for Women’s Health Research and work within these agencies to establish innovative programs to expand access to care and services (e.g., a Federal Access to Contraception Program to address gaps in access for those whose employers may not offer contraceptive coverage).
- Establish permanent Infertility Benefits for Active-Duty Members of the U.S. Military, Veterans, and Employees of the Veteran’s Administration.
GOAL II: ADDRESS UNIQUE BARRIERS TO REPRODUCTIVE MEDICINE FOR SPECIFIC POPULATIONS
Overview of Barriers in Access to Care
Only one in four people get the treatment needed to overcome infertility. 10 Cost is the #1 barrier to care.11 The average cost of an IVF cycle in the United States is approximately $15,000.12 A recent survey found that women (25-34 years old) accrued, on average, around $30,000 of debt after undergoing fertility treatment. Such costs put fertility treatment out of reach for many, and especially those in the Black and Hispanic communities, as reported by the Kaiser Family Foundation Report on Coverage and Use of Fertility Services in the U.S.13 The LGBTQ community also faces additional obstacles, including when insurers define infertility based on sexual intercourse.ASRM is committed to addressing the factors that impact health disparities in our subspecialty and to addressing the ability of individuals to access proper and equitable medical care, which is a pervasive barrier to educational, economic, and social success.
Barriers to Care for LGBTQ Individuals
Unmarried individuals, and many in the LGBTQ community face extra barriers to building their families. Some face discrimination based on their sexual orientation, and some cannot meet narrow, heteronormative definitions of infertility that link coverage to attempts at pregnancy within a partnered, heterosexual relationship.13
In addition, transgender individuals may wish to preserve their gametes before undergoing gender-affirming treatments. Such services could be viewed as akin to those with iatrogenic infertility or other conditions and diseases (like cancer), but discrimination and cost may still present obstacles to care.
We must act to reduce and address infertility-related stigma in diverse populations. The Biden Administration should embrace opportunities to expand outreach to the LGBTQ community on the issue of infertility, and advance efforts to provide education on early identification and local family building resources in hopes of reducing stigma in these communities.
Barriers to Care for People of Color
Physicians are human and their human experience absolutely influences the way in which they practice medicine and treat their patients. Unfortunately, this means they may consciously or unconsciously make assumptions or act on biases about who deserves to be a parent and who needs or deserves treatment. These implicit biases can lead to discrimination in provision of care and in health outcomes for patients, contributing to health disparities.15 Women of color, for example, have reported that some physicians brush off their fertility concerns, make assumptions that they can get pregnant easily, emphasize birth control over procreation, and may dissuade them from having children altogether.16 These biases come from painful, historically rooted societal stereotypes about sexual activity, sexual risk, motherhood status, and socioeconomic status.17
According to ASRM’s DEI Task Force, research on IVF outcomes and race/ethnicity, including three studies using data collected by the Society for Assisted Reproductive Technologies (SART), suggests that when African American, Asian, and Hispanic women attain access to ART, they experience lower success rates compared with non-Hispanic white women.18 The fi ndings include evidence of lower implantation and clinical pregnancy rates, as well as increased miscarriage rates among certain minority women. These differences in treatment success are concerning; they are poorly understood and insuffi ciently studied, with explanations ranging from biological factors to modifi able behavioral factors.19-21 Their rectifi cation is critical to achieving reproductive health equity among women and men of color. Additional research is urgently needed to identify the causes and the remedies for these disparate outcomes.
Barriers to Care for Service Members
Due to a Congressional ban enacted in 1992, the Department of Veteran’s Affairs (VA) has since specifically excluded IVF coverage from the VA medical benefits package. Similarly, TRICARE, which provides health benefits to active-duty members, does not cover IVF. In 2016 Congress authorized coverage of IVF for veterans whose infertility is caused by a service-connected injury. This was reauthorized in 2018 and must be reauthorized annually, or it lapses. Even when veterans demonstrate that their infertility is causally linked to active-duty service, there are further restrictions to exclude those who are not legally married and require the use of donor gametes. Effectively limiting coverage to only partnered, heterosexual individuals.23
The VA does offer certain types of fertility services to veterans including infertility counseling, laboratory blood testing, surgical correction of structural pathology, reversal of a vasectomy or tubal ligation, medication, and various other diagnostic studies or treatments and procedures.
The Military Health System does provide general infertility services through the private sector under the TRICARE Basic Program. This is limited to services and supplies which are medically necessary to diagnose or treat a physical illness, injury, or bodily malfunction and does not include coverage for IVF treatment. In 2013, the DoD was authorized to provide access to IVF for those with service-connected infertility. Due to the strict requirements, in the first two years, only 20 members met the criteria to utilize this benefit.
Meeting the reproductive healthcare needs of service members is critical to ensuring military readiness and mission accomplishment. It is a moral imperative that we provide the best quality care to facilitate family building to those who sacrifice so much to protect the health and safety of our country.
Barriers for Those At-Risk of Iatrogenic Infertility
In the United States, approximately 132,350 individuals between ages 0-45 are diagnosed with cancer each year.24 As cancer survivorship improves, these patients face good odds; approximately 80% will survive. Chemotherapy, radiation, and surgery can cause medically induced (iatrogenic) infertility by damaging gametes (eggs and sperm), reproductive organs, and/or endocrine functioning; they also may impact the ability to carry a pregnancy. Patients with other conditions requiring similar therapies (e.g., sickle cell disease (SCD), lupus, and thalassemia, etc.) are also at risk.25 SCD affects approximately 100,000 patients per year in the U.S. These patients are increasingly being recommended for stem cell transplants, which, while curative, are highly toxic to the reproductive system and usually sterilizing.In many cases, patients at-risk of iatrogenic infertility are given very short notice before beginning treatment that could render them infertile. Unfortunately, ASRM has heard of instances, particularly in California, where insurance companies who claim they cover fertility preservation, have not done so. As such, ASRM encourages Congress to codify the enforcement of fertility preservation coverage for patients at-risk of iatrogenic infertility.
Barriers for Providers
The lack of diversity of reproductive care providers is a major barrier when it comes to equitable access to care. As of December 2018, there were 50 ACGME approved reproductive endocrinology & infertility (REI) fellowship programs. Of 156 total reproductive REI fellows in the programs at the time, just 11 (7%) identified as Black/African American, five as Hispanic/Latino (3.2%), 22 as Asian (14.1%), and six as Multiracial.26 Demographic data on the racial/ethnic diversity of other reproductive care practitioners, including practicing REIs, reproductive care nurses, mental health professionals, laboratory personnel, or laboratory directors, could not be found.
In recognition of this dynamic, and related challenges, a primary charge of the ASRM DEI Task Force was to make recommendations for enhancing opportunities to increase and support diversity and equity, and the inclusion of underrepresented populations, both in the profession and leadership of reproductive medicine.
Moreover, the Administration should evaluate opportunities to increase reproductive health education for students in middle and high schools, colleges and universities, medical schools and postgraduate medical training, including REI fellowships. The goal would be to encourage students of color and diverse ethnicities, religious beliefs, and gender identities to pursue careers as physicians, nurses, biologists, and in other reproductive health disciplines to develop a more diverse reproductive health workforce.
The federal government should lead and support efforts to engage in outreach to identify diverse talent across all levels of the field of reproductive medicine. This should include development of pipeline programs to increase diversity throughout all provider specialties.
The Administration should invest in efforts to develop and deliver specific training to minimize implicit bias, stereotyping, discrimination, and racism, and make a requirement for all REI training directors, faculty, and trainees, to attend mandatory cultural sensitivity training. An investment to expand and enhance training to support a diverse and informed workforce will have long-term benefits for Americans across the board.
Policy Recommendations to Address Unique Barriers to Reproductive Medicine for Specific Populations
- Pass a National mandate to enforce insurance coverage for fertility preservation for those at-risk of iatrogenic infertility
- Develop and implement HHS/DOJ/EEOC rule to protect “special” populations from discrimination in infertility coverage
- Increase funding for increase reproductive health education for students in middle and high schools, colleges and universities, medical schools and postgraduate medical training
- Fund and require cultural bias and sensitivity training for all medical providers
GOAL III: INCREASING THE NATIONAL INVESTMENT IN REPRODUCTIVE MEDICINE RELATED RESEARCH
Reproduction is a fundamental part of human experience. Even the United States Supreme Court has described it as a “major life activity.”27 As in many other economically developed countries, the birth rate in the United States has been falling in recent years. While there are of course significant social reasons for this decline, there also are medical ones. In order to have a healthy, economically vibrant society, population levels must be maintained. A declining birth rate can put tremendous economic pressure on up-and-coming generations to generate sufficient economic activity to support retirees. Perhaps even more importantly, the psychological distress that accompanies infertility has been found to be on a level, or even stronger, than that which cancer patients face.
While there have been tremendous advances in reproductive medicine in recent years, there is still much we do not know. For example, the process of implantation of a fertilized egg into the uterus in order to initiate a pregnancy remains one of human biology’s greatest mysteries. We understand more and more the importance of the earliest stages of human development on later health outcomes; and we have an increasing awareness of the impact of pre-conception health and the health of the gametes, sperm and eggs, on later human health. Sadly, while we are gaining an awareness of its importance, there is still much about it we do not understand—specifically about how to improve reproductive outcomes.
Some of it is simply inadequate funding. The National Institute of Child Health and Human Development (NICHD), the part of the National Institutes of Health which provides much of the support for reproductive-related research typically lags behind other components of the NIH when it comes to funding, particularly for investigator-initiated funding. To add insult to injury, in recent years Congress has appropriated funds directly to the NIH Office of the Director to such an extent that its budget now exceeds that of NICHD.
Moreover, this year, Congress overlooked the NICHD, even as it provided new funding to support the NIH and many of its institutes and centers as they work through the unique challenges--and research opportunities--presented by the COVID-19 pandemic.
NICHD has made extraordinary achievements in meeting the objectives of its biomedical, social, and behavioral research mission, including research on reproductive biology; women’s health throughout the life cycle; maternal, child, and family health; learning and language development; population health; and medical rehabilitation. Moreover, the World Health Organization and the Centers for Disease Control and Prevention have each articulated the increased risk of COVID-19 to people with disabilities. The NICHD is well equipped with a network of researchers, including IDDRCs, to address the impact of COVID-19 on these high-risk populations.
Despite the lack of new funds this Fiscal Year, NICHD is an active participant in the COVID-19 response at NIH. The NICHD has been an active participant in NIH Institute and Center-wide discussions on the topic, including working to ensure that NICHD’s populations are included in COVID-19 related research (e.g., vaccine and therapeutic clinical trials). Additionally, NICHD’s experts are exploring options to repurpose funds to support a pregnancy registry to better understand maternal and neonatal outcomes for pregnant people with COVID-19 and their infants. Moreover, NICHD is supporting efforts to leverage the trans-NIH Pediatric Research Consortium (N-PeRC) to cultivate pediatric and obstetric research ideas and collaboration in the wake of COVID-19.
NICHD is taking on these key efforts even as it maintains a robust and critical research portfolio, which addresses topics including, but not limited to, maternal mortality; infant and childhood health; behavioral health; poverty and child health; reproductive sciences; healthy pregnancies; and human development from infancy through adulthood. We implore the Biden Administration to increase the Federal investment in this Institute’s critical and unmatched work.
Politics as an Historic Impediment to Progress
We at ASRM, support people refusing medical treatments they find ethically troubling; we cannot, however, support their stopping the rest of us from improving our understanding of human reproduction in order to alleviate suffering.
The first in vitro fertilization (IVF), a procedure that was later recognized with a Nobel Prize, was first performed in the United Kingdom, not the United States. This, even though much of the foundational work was performed by U.S. Scientists in U.S. laboratories. The sad fact is that politics got in the way. A trend that has unfortunately continued.
The federal government has never funded research involving a human embryo.
With the advent of the first IVF in 1978, the United States government began exploring the ethics of federal funding for human embryo research. After an exhaustive review, which included town hall meetings all over the country, it was recommended that a special ethics panel be created to guide the process at NIH. After the Presidential election of 1980, the Reagan, and then George H.W. Bush administrations simply never empaneled that group, thus enacting a de facto ban on human embryo research. The Clinton administration took another look at the issue and opted to pursue a policy that would allow federally funded investigators to work with human embryos, but not to create them for research purposes. However, before this policy could be enacted, Congress added a rider to the FY 1996 Appropriations Bill banning HHS from using federal funds for human embryo research. A policy rider that survives to this day.
As we entered the 21st century, advances in embryology allowed the in vitro embryo to be cultured in the lab for a longer period, approaching five days when the embryo has developed into a 100-cell blastocyst. Cells from the blastocyst have the potential to become any kind of cell in the body. Researchers were eager to exploit this capacity to develop tissues which could be used to alleviate several devastating conditions. Federal support, or more accurately, lack thereof, for embryo research became a hot political issue. In August 2001, President George W. Bush announced a policy that would allow NIH to fund work using already existing stem cell lines, but not to create new ones. During the remainder of the Bush years, Congress twice passed legislation lifting this restriction only to see the President use his veto powers to block it.
In 2009, President Obama revisited the embryonic stem cell policy, ultimately lifting the blanket restrictions and allowing NIH to develop standards. These focused on ethical review of the procurement of stem cells. In more recent years, other issues and restrictions have emerged. As gene editing techniques advanced, investigators began to speculate on their application to gametes and embryos. This could, for example, eliminate a disease like sickle cell anemia for a family for all subsequent generations. However, rather than rely on the robust review system required of any new medical materials, Congress decided without review or committee deliberation, to cut off this line of inquiry and not allow the FDA to even entertain an application to review the science for safety and efficacy. Finally, taking on a debate which had been settled in the 1990s the Trump administration began to restrict federal support for research that involved fetal cell lines, ultimately, requiring a new special review and empaneling a committee that so far has approved only a single protocol. In order to advance our understanding of human reproduction, to better treat reproductive disorders, and perhaps to use the power of reproductive cells and tissues to provide for relief of a host of human ailments, we need to lift these politically imposed restrictions and let America’s scientists get to work.
Recommendations to Increase the National Investment in Reproductive Medicine-Related Research
- Increase funding for research in human reproductive disorders. Specifically, increase funding for the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD).
- Lift the prohibition on human embryo research and allow the National Institutes of Health (NIH) to develop oversight of the ethics of research proposals.
- Protect, through Congressional codification, access to embryonic stem cell lines.
- Protect, through Congressional codification, access to fetal cell lines.
- Authorize the FDA to examine the data of any proposed germ line gene editing techniques.
CONCLUSION
Sean Tipton
ASRM Chief Advocacy Policy and Development Officer
stipton@asrm.org
References
- See RESOLVE survey, 2007 and subsequent: www.RESOLVE.org
- Stanley, M.; Foti, T., Health Insurance for Infertility Services: It’s About Where Your Work, More than Where You Live (2020).
- Weigel, Gabriela; Ranji, Usha; Long, Michelle; Salganicoff, Alina. Coverage and Use of Fertility Services in the U.S. (Kaiser Family Foundation Issue Brief, Sept. 15, 2020). https://www.kff.org/womens-health-policy/issue-brief/coverage-and-use-of-fertility-services-in-the-u-s/?utm_campaign=KFF-2020-Womens-Health-Policy-WHP&utm_medium=email&_hsmi=2&_hsenc=p2ANqtz-9tBIocfJBDrFL4lgyIhXbqjaxLrQDmBOma02mlpFIcATdbN9vG_Eil_cQQZgLpcN_-jlzpp2wfHzU7DMo-vPcQpOZvSQ&utm_content=2&utm_source=hs_email
- American Society for Reproductive Medicine Ethics Committee. Disparities in access to effective treatment for infertility in the United States. (Ethics Committee Opinion, Updated 2020).
- See, Armstrong, 2012; Bell 2010; Cordasco 2011; Inhorn 2005; McCarthy 2010.
- See, Wu 2013; Missmer 2011; Domar 2018.
- See, Nachtigall, 2009.
- ASRM Ethics Committee, Access to Fertility Treatment by Gays, Lesbians, and Unmarried Persons. (Committee Opinion). Fertil Steril 2013;100:1524–7.
- Weigel et al. Coverage and Use of Fertility Services in the U.S. (Kaiser Family Foundation Brief, Sept. 15, 2020).
- American Society for Reproductive Medicine, White Paper: Access to Care Summit, September 10 - 11, 2015 Washington, D.C.
- “Cost.” FertilityIQ, www.fertilityiq.com/topics/cost.
- Marketplace, Prosper. “Fertility Treatments in the United States: Sentiment, Costs and Financial Impact.” Prosper Blog, 20 May 2015, www.prosper.com/blog/2015/05/20/fertility-treatments-in-the-united-states-sentiment-costs-and-financial-impact/.
- Wiegel, Gabriela et al. Coverage and Use of Fertility Services in the U.S., Published by Kaiser Family Foundation: Sep 15, 2020.
- Ada C. Dieke et al., Disparities in Assisted Reproductive Technology Utilization by Race and Ethnicity, United States, 2014: A Commentary, 26 J. WOMEN’S HEALTH 605 (2017), https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5548290/
- Shavers VL, Fagan P, Jones D, Klein WM, Boyington J, Moten C, Rorie En Am J Public Health. 2012 May; 102(5):953-66.
- Bell AV. Beyond (fi nancial) accessibility: inequalities within the medicalisation of infertility.Sociol Health Illn 2010;32:631–46.
- Rosenthal, Lisa, and Marci Lobel. “Stereotypes of Black American Women Related to Sexuality and Motherhood.” Psychology of women quarterly vol. 40,3 (2016): 414-427. doi:10.1177/0361684315627459
- Armstrong A, Plowden TC. Ethnicity and assisted reproductive technologies. Clin Pract (Lond) 2012;9:651–8.
- Humphries LA, Chang O, Humm K, Sakkas D, Hacker MR. Influence of race and ethnicity on in vitro fertilization outcomes: systematic review. Am J Obstet Gynecol. 2016;214:212.e1-212.e17.
- McQueen DB, Schufrieder A, Lee SM, Feinberg EC, Uhler ML. Racial disparities in in vitro fertilization outcomes. Fertil Steril 2015; 104:398-402.
- Kelley AS, Qin Y, Marsh EE, Dupree JM. Disparities in accessing infertility care in the United States: results from the National; Health and Nutrition Examination Survey, 2013-2016. Fertil Steril 2019; 112:562-68.
- Service Women’s Action Network, Access to Reproductive Health Care: The Experiences of Military Women (2018), https://www.servicewomen.org/wp-content/uploads/2018/12/2018ReproReport_SWAN-2.pdf .
- Access to IVF for Servicemembers and Veterans (fact sheet), Center for Reproduction Rights (2020), https://reproductiverights.org/document/access-ivf-servicemembers-and-veterans
- Center for Disease Control and Prevention. United States Cancer Statistics: Data Visualizations. https://gis.cdc.gov/Cancer/USCS/DataViz.html. (2017). Accessed June 8, 2018.
- Katsifis GE TA. Ovarian failure in systemic lupus erythematosus patients treated with pulsed intravenous cyclophosphamide. Lupus. 2004;13:673-678; Rovoa, T., Passweg J., Heim D., Meyer-Monard, S. HW. Spermatogenesis in long term survivors after allogenic hematopoietic stem cell transplantation is associated with age, time interval since transplantation, and apparently absence of chronic GVHD. Blood. 2006;108(3):1100
- Bell AV. Beyond (fi nancial) accessibility: inequalities within the medicalisation of infertility. Sociol Health Illn 2010;32:631–46.
- Bragdon v. Abbott, 524 US 624 (1998), at 10.